The following case study was used by Andrew J. White, MD, the James P. Keating, MD, Professor of Pediatrics and division director of pediatric rheumatology, Washington University School of Medicine, and director of the St. Louis Children’s Pediatric Residency Program, as part of the “Patient of the Week” (POW) series. Many of the POW case studies cover uncommon illnesses, or common illnesses with unusual symptoms that can be overlooked. If you would like to be added to the POW e-mail distribution, send an email to [email protected].
This case was submitted by Saquib Lakhani, MD, (SLCH Resident 1996-1998), who is now in Pediatric Critical Care, Sanford School of Medicine at the University of South Dakota.
3-year-old boy with CC: “mood spells.”
He is a healthy boy who six months ago began having “mood spells.” They occur on average once a week, though frequency has increased to about every other day over the past month. They typically begin with an odd comment, which alerts parents that an episode of moodiness is about to begin. Mother pulls out a camera and shows a video to the physician.
Episode description: He was sleeping in the back seat of the minivan when he abruptly sat up, exclaimed, “Mom, is it ok if I sleep?” and began staring. When the recording begins he is sitting upright looking hyper alert and a bit worried when he suddenly begins laughing uncontrollably and almost maniacally. This lasts for about 20 seconds and then he begins tearfully sobbing for another 5-10 seconds. After this he lays his head on the armrest and promptly falls asleep.
Parents report that this recorded episode is fairly typical and he usually sleeps for at least an hour and up to a few hours after each spell. The spells have no specific trigger. The spells are not interruptible; they simply run their course. He had a normal routine EEG a few weeks ago, though he did not have a spell during the EEG.
Exam:
Afebrile, normal vital signs for age. Awake, pleasant child in no distress. Heart with regular rhythm, no murmurs. Pulses 2+. Lungs clear with good aeration. Abdomen soft, nontender. No hepatosplenomegaly.
Neuro: Alert and appropriately interactive. Cranial nerves II-XII intact. Good strength, tone, reflexes and coordination.
A diagnostic test was obtained:
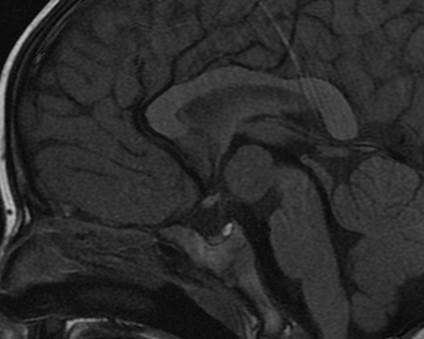
MRI Brain:
There is a 1.5 x 1.7 x 1.7-cm mass centered at the level of the floor of the third ventricle in the region of the tuber cinereum. The signal of the mass follows gray matter on all pulse sequences and there is no associated enhancement on post contrast images. The optic tracts are located just lateral to the mass on each side and the mammillary bodies are located just inferior to the mass.
There is no diffusion abnormality. No evidence of intracranial hemorrhage. No hydrocephalus. The major intracranial flow voids are intact. There is no abnormal enhancement identified. The hippocampal formations appear normal with no evidence of mesial temporal sclerosis. The sulcal and gyral pattern appears symmetric and within normal limits. No evidence of a migrational abnormality. The posterior fossa structures appear normal.
Impression:
Mass at the floor of the third ventricle centered at the tuber cinereum of the hypothalamus, most likely a hamartoma.
Diagnosis:
1. Hypothalamic hamartoma
2. Gelastic seizures, secondary to #1 (Gelos = Greek for laughter)
Treatment: Surgical resection vs. thermocoagulation vs. gamma knife therapy (for which he is currently being evaluated).
Neither levetiracetam nor valproic acid seem helpful in controlling his seizures, but symptoms typically do improve/resolve with resection of the mass.
He has no signs of precocious puberty (known to occur in this syndrome).
The mechanism of the laughter is unknown.








