Background
 Brachial plexus palsy is caused by a birth injury to the brachial plexus, the nerve network that controls movement and sensation of the arm. The main result of this injury is weak or paralyzed muscles in the shoulder, arm, and hand. Fortunately, most infants with this condition make complete spontaneous recovery. Some, however, are left with varying degrees of arm weakness.
Brachial plexus palsy is caused by a birth injury to the brachial plexus, the nerve network that controls movement and sensation of the arm. The main result of this injury is weak or paralyzed muscles in the shoulder, arm, and hand. Fortunately, most infants with this condition make complete spontaneous recovery. Some, however, are left with varying degrees of arm weakness.
Among infants who do not recover spontaneously, some will require physical therapy and occupational therapy only, and others will need both therapy and surgery. Children who develop deformities in the shoulder, arm, or hand may need orthopaedic treatment. In all cases, treatment must be started early to ensure the greatest improvement.
Brachial plexus palsy is diagnosed in the newborn nursery. Primary physicians need to identify and refer patients to the multidisciplinary brachial plexus team. During the first 2-6 months after birth, the following specialists on the team work together to restore normal functioning in the infant's arm.
obstetrician/pediatrician
makes diagnosis
pediatrician
refers infant to the Brachial Plexus Center
neurologist and neurosurgeon
determine whether an infant is likely to recover completely or to need surgery
neurosurgeon
performs necessary neurosurgery
physical and occupational therapists
assess arm function
perform treatment to maximize improvement in arm function
instruct parents in home exercise techniques
orthopedic surgeon
provides surgery for children older than one year who develop deformities in the shoulder, arm, or hand
parents
perform range of motion exercises with infant at home
This web site provides up-to-date information for parents, physicians, therapists, and nurses about birth brachial plexus injury and its management. The information is based on medical reports and our own clinical experience, and we are solely responsible for its accuracy. Please address any questions regarding this web site to:
Brachial Plexus Center
St. Louis Children's Hospital, Room 4S 20
One Children's Place
St. Louis, MO 63110-1077
Phone: 314.454.2811; Fax 314.454.2818
email: [email protected]
Reports in the Literature
|
History of Documentation of Obstetrical |
||
|
Smellie (1768): |
First Documentation | |
|
Duchenne (1872): |
Mechanism of Injury | Traction during Birth |
|
Erb (1874): |
C5 - 6 nerve root injury | "Erb's Palsy" |
|
Klumpke (1885): |
C8 - T1 Injury | "Klumpke's Palsy" |
|
Sever (1925): |
"Surgery plays no role" | |
|
Gilbert & Tassin (1987): |
Rejuvenated interest in Surgery | |
Injury to the brachial plexus at birth has probably always occurred. The first recorded mention of it is by William Smellie in a 1768 publication on midwifery.
In the late 19th century, French neurologist Guillaume Duchenne described the cause of injury as traction on the arm and shoulder during birth. Around the same time, German neurologist Wilhelm Erb identified the nerves damaged and the muscles affected (weakness in the deltoid, biceps, coracobrachialis, and brachioradialis muscles caused by disruption of the C5 and C6 nerve roots - see Anatomy section). The disorder, known as Erb's palsy, involves an extended, internally rotated arm, flexed wrist, and extended fingers (posture known as "waiter's tip hand"). A much rarer disorder is Klumpke's palsy, in which a different part of the nerve plexus is damaged (C8-T1 nerve roots), affecting muscles of the hand and also the pupil of the eye on that side.
Surgery for birth brachial plexus was first reported in the early 1900s. However, in the first part of this century, surgical treatment was so often unsuccessful (see Sever's 1925 report on 1,100 cases), with high rates of associated problems and even death, that it was almost abandoned. With the development of microsurgical nerve grafting techniques in the 1970s, surgical treatment of traumatic brachial plexus injuries was resumed in adults. The last decade has seen the development of effective surgical treatment for infants.
Prevalence
|
How common is Birth Brachial Plexus Palsy? |
|
|
Total Prevalence: |
0.2 - 2.5 / 1,000 births |
|
Persistent Weakness: |
0.4 - 5.0 / 10,000 births |
The estimated prevalence of birth brachial plexus injury ranges from 0.2 to 2.0 per 1,000 births, and significant arm weakness persists in 0.4 - 5.0/10,000 births.
A wide range in the prevalence and persistence of arm weakness due to brachial plexus injury has been reported. This variability is probably a reflection of the patient population treated at individual centers. For instance, a referral center sees the worst injuries and would probably underestimate the prevalence of the birth brachial plexus injury and overestimate the relative persistence of weakness. It should be noted, however, that improvement of obstetrical care has not eliminated birth injury, mainly because of inherent risk factors (described in the next section).
Pathogenesis
The brachial plexus is injured by traction on the shoulder during delivery. Infants affected are usually large, so that it is necessary to use force in pulling them from the birth canal. When the shoulder is forcibly pressed downward, the brachial plexus can be stretched or injured.
The type of delivery correlates with the type of brachial injury. According to one report, infants with upper brachial plexus injury (Erb's palsy) are more likely born by breech delivery, and those with more extensive injury are more likely born headfirst. However, brachial plexus palsy can occur even with cesarean section.
|
Delivery and Types of Brachial Plexus Injury |
|
|
Breech delivery: |
73% of C5-6 injuries |
|
Cephalic delivery: |
88% of C5-7 injuries 96% of C5-T1 injuries |
In certain infants, problems exist before birth that cannot be anticipated or corrected by the obstetrician. Examples of risk factors are
- large size (weight more than 8 lb 13 oz)
- breech delivery
- mother with many previous deliveries
- prolonged second stage of labor
- maternal obesity
- prolonged pregnancy (more than 42 weeks)
- maternal diabetes
- midpelvic operative delivery
- vacuum or forceps delivery
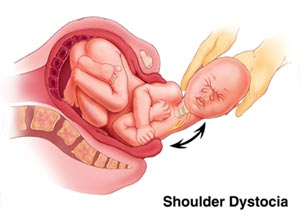
These factors increase the chance of shoulder dystocia, which is damage that occurs when the infant's shoulders are entrapped in the birth canal during delivery.
A mother who has had one child with brachial plexus injury is at significantly greater risk than the general population for having another child with the same disorder.
Types of Injury
Upper Brachial Plexus (Erb's) Palsy
In this condition, the upper part of the nerve plexus is damaged. Along with total brachial plexus palsy, this is the most common form of the disorder. These infants cannot move the shoulder and keep their arms extended and turned inward, giving the appearance of the "waiter's tip hand." Often, these babies have no movement of the arm right after birth but begin to move the fingers and wrist within a few weeks. The weak shoulder and elbow movement remain persistent problems, however.
Total Brachial Plexus Palsy
In these infants, the entire brachial plexus is affected. Infants with total brachial plexus injury have no movement of the arm, wrist, or hand; the arm is limp. This type of injury is more often associated with nerve roots being detached from the spinal cord, which is more difficult to treat.
Lower Brachial Plexus Palsy
Isolated lower plexus injury is exceedingly rare, and we have not encountered such a case. Typically the lower brachial plexus is involved as part of a more extensive injury, such as total brachial plexus injury.
Bilateral Injuries
The brachial plexus can be injured on both sides of the body, although such cases are rare. Bilateral injuries can be mistaken for other problems, such as spinal cord injury.








