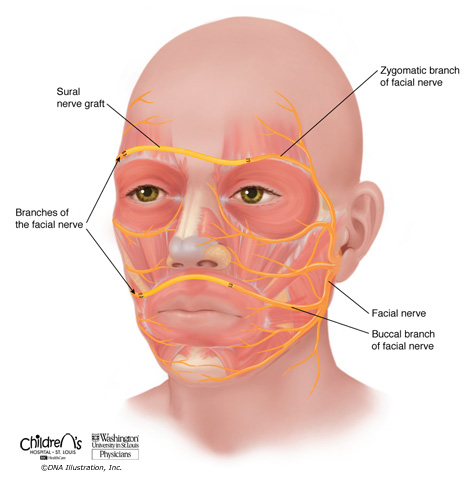
Figure A: Cross-facial nerve graft.
When facial paralysis affects only one side of the face, early reconstructions may borrow a specific branch or branches of the facial nerve from the unaffected side of the face to reconstruct movement. A nerve graft, which acts similar to an extension cord, is required, and nerve fibers slowly grow from the unaffected side of the face across the nerve graft to the paralyzed side of the face. Click to enlarge.
Reconstructions are tailored to each person’s unique circumstance. It is important to realize that facial nerve reconstructions rarely result in an appearance identical to the pre-injury state or similar to a person unaffected by facial paralysis, although this is the goal. While it is not possible to recreate all of the intricate movements of facial expression, many excellent techniques are available for smile reconstruction. Reconstructions do typically improve facial function, balance, and appearance, although success is never guaranteed. Achieving greater symmetry and the individual’s personal goals are emphasized.
Early Reconstruction
Reconstructions performed early after facial nerve injury are often able to preserve the original muscles of facial expression. Other nerves may be used to power the muscles if the facial nerve is not available.
Direct Nerve Repair
If the facial nerve has been cut, it may be able to be directly repaired, particularly if managed within a few days from the injury. These injuries often require a nerve graft, or a segment of another nerve, usually the sural nerve from the calf, to span a gap between the two cut ends.
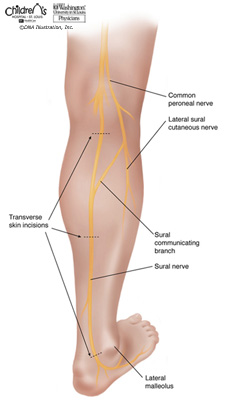
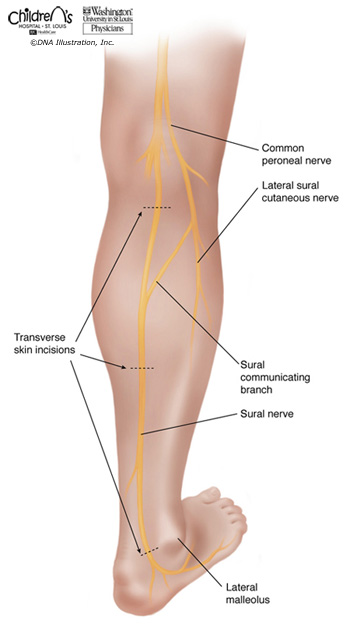
Figure B: Sural nerve harvest.
The sural nerve is located in the calf and provides sensation (feeling) to the lateral side of the foot. The sural nerve is commonly used as a nerve graft. The nerve is removed via two or three scars on the back of the leg, shown as the dashed lines. The sural nerve is expendable and is not required for walking. Click to enlarge.
Cross-Facial Nerve Grafts
(See Figure A) In cases of paralysis affecting only one side of the face, the normal, unaffected facial nerve on the opposite side may provide a source of nerve fibers. Specific extra facial nerve branches from the healthy side of the face can be identified and connected to the paralyzed side of the face with a nerve graft. The nerve fibers then grow from the healthy facial nerve, across the nerve graft, and to the dysfunctional nerve and paralyzed muscles. The nerve graft acts somewhat like an extension cord, however, it takes time (months) for the nerve fibers to grow across the face to reach their target.
Typically the sural nerve in the calf is used as the nerve graft (See Figure B). The sural nerve is an expendable sensory nerve. It is removed from the leg via two or three small incisions. A numb patch on the outer side of the foot remains after the sural nerve is removed from the leg. This nerve is not required for walking.
Nerve Transfers
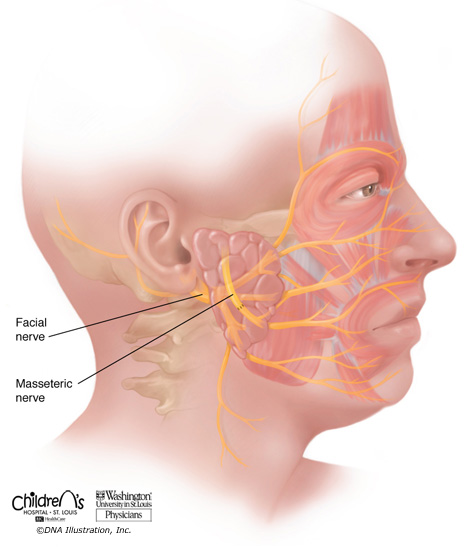
In cases of paralysis affecting both sides of the face, there is not a healthy facial nerve available to borrow from. Other nearby nerves can be used to provide a nerve source for the facial muscles. A branch of a nerve utilized in chewing, the masseteric nerve, is commonly utilized (See Figure C). This nerve branch is expendable, and its use does not result in chewing difficulties. The masseteric nerve branch can be connected to the affected facial nerve. This nerve transfer does not require use of a nerve graft, meaning no surgery is required in the leg. Therapy is required after surgery for the child to learn how to use this nerve for facial movement.
Figure C: Masseteric nerve to buccal nerve coaptation.
The masseteric nerve, normally used in chewing, can provide a nerve supply for facial expression in early reconstructions when the muscles of facial expression are healthy, but the facial nerve is not available. The masseteric nerve can be connected to the remaining end of the facial nerve. Click to enlarge.
Later Reconstruction
For people with long-standing facial paralysis (greater than 12-24 months), substitution of the nerve supply alone is not sufficient. In these circumstances the original muscles of the face can no longer accept a nerve, and alternative muscles are also required for movement. Muscles from other regions of the body may be utilized. Static reconstructions may be performed to provide support to the face.
Static Reconstructions
Static reconstructions act as an internal sling for the face. They provide support, but not movement. Static support slings may be constructed from other regions of the body, such as fascia from the thigh, forearm, or temple, or from surgical products. Static techniques are sometimes used in combination with dynamic reconstructive techniques.
Dynamic Reconstructions
There are many techniques for reconstructions that provide movement to the paralyzed face. Some examples are listed below:
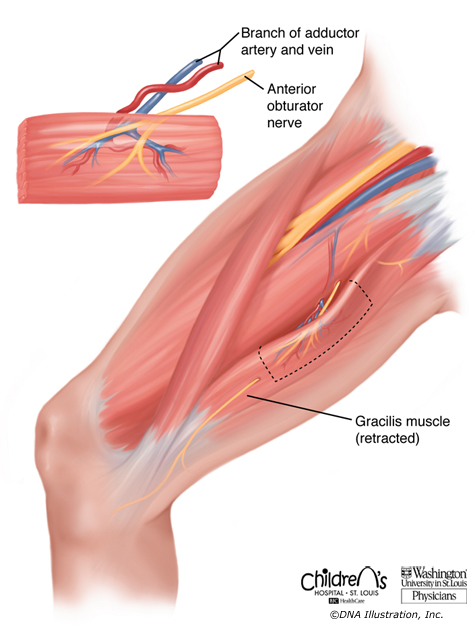
Figure D: Segmental gracilis harvest
A portion of the gracilis muscle can be moved from the inner thigh to the face to provide the smiling motion. The muscle is moved with its blood vessels (so that it is alive) and its nerve (so that it may move). Removal of the muscle from the thigh does not cause problems with walking, running, or use of the leg since multiple other muscles provide the same movement. Click to enlarge.
Regional Muscle Transfers
Functioning muscles on the paralyzed side of the face, such as muscles involved in chewing that are innervated by the trigeminal nerve (cranial nerve V), can sometimes be partially moved to provide facial movement.
Free Functional Muscle Transfers
Advances in microsurgical techniques have made free functional muscle transfers reliable and more elegant. A segment of a muscle from another body region can be transferred to the face to provide movement. The gracilis muscle is an expendable muscle from the inner thigh which is well-suited for transfer to the face (see Figure D). Removal of this muscle from the thigh does not decrease leg movement as four additional muscles perform its same task. The muscle segment is transferred with its blood vessels (so that it is alive) and its nerve (so that it may move). The blood vessels and nerve are then connected to blood vessels and a nerve within the face. The muscle is positioned so that when it contracts, it provides a smiling movement to the corner of the mouth and upper lip.
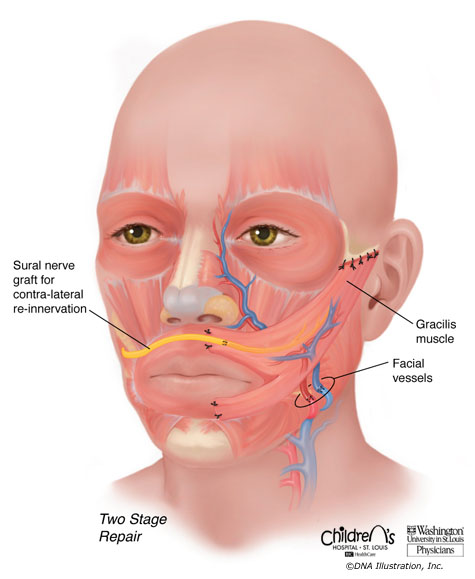
Figure E: Free functional muscle transfer with cross-facial nerve graft.
For later reconstructions, facial movement is produced with new muscle and new nerve. A segment of the gracilis muscle from the thigh is positioned in the face to provide smiling motion. The cross-facial nerve graft, which connects to the facial nerve on the unaffected side of the face, can power the transferred muscle. This procedure is performed in two stages, with surgeries often spaced 6-12 months apart. Click to enlarge.
This procedure is technically very demanding and requires the use of microsurgery to connect vessels with sutures (stitches) several times thinner than human hairs. This reconstruction may be performed in one or two surgical stages, depending on the nerve supply that will be used. We most commonly use this technique in combination with a cross-facial nerve graft and the facial nerve on the opposite face (two stages) with CFNG/VII (see Figure E) or a masseteric nerve transfer (one stage) (see Figure F). For both of these nerve sources, the donor nerve (either the graft or the masseteric nerve) is connected to the nerve to the gracilis muscle (the obturator nerve). The nerve fibers then slowly grow into the transferred gracilis muscle to allow it to contract over time, usually in 4-9 months or more. For bilateral reconstructions, a gracilis muscle can be transplanted to each side of the face. We prefer to do this in two separate surgeries, usually at a minimum of 3 months apart.
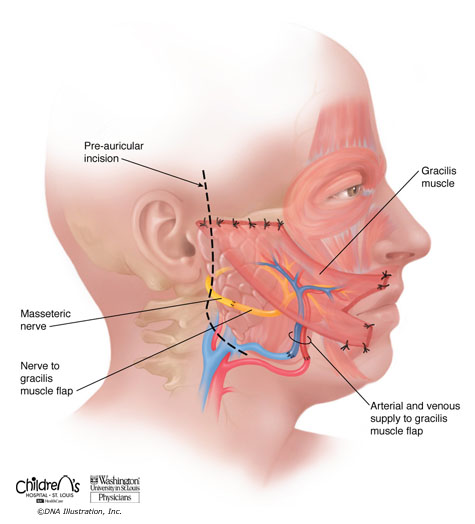
Figure F: Free functional muscle transfer with masseteric nerve.
For later reconstructions, facial movement is produced with new muscle and new nerve. A segment of the gracilis muscle from the thigh is positioned in the face to provide smiling motion. The masseteric nerve, normally used in chewing, can power the transferred muscle in a single-stage technique. The scar for this procedure is depicted with the dashed line. Click to enlarge.
Many families have to adjust when young adult children live at home. Clear expectations, shared responsibilities, and healthy communication support
...