When is hemispherotomy offered?
Hemispherotomy may be offered to children with refractory seizures arising from one hemisphere of the brain, particularly if there is already a suggestion of impaired function of that hemisphere (such as weakness of the opposite side of the body).
In some instances, hemispherotomy may be offered to treat life-threatening seizures, such as status epilepticus, or those causing significant ongoing neurological damage, even if the opposite side is not entirely normal.
Experts at hemispherotomy
The Pediatric Epilepsy Team at St. Louis Children’s Hospital has extensive experience with hemispherotomy. In fact, our experience has been highlighted at several national and international meetings.
The hemispherotomy procedure
Our current surgery for hemispherotomy is a modified version of a technique called peri-insular hemispherotomy.
The steps of the procedure are as follows:
- A small question-mark-shaped incision is made above the ear on the affected side.
- A section of bone is removed which will provide access for the remainder of the operation.
- A natural division between the frontal and temporal lobes is opened, and a small amount of each of these lobes is then removed.
- Using the guidance of special MRI scans and a navigation computer, the cerebrospinal fluid cavity (ventricle) is opened, exposing the deeper structures of the brain.
- The amygdala and hippocampus are removed from the temporal lobe, and a division is made in the corpus callosum, which is a band of fibers connecting the two hemispheres.
- The disconnection is then completed in the frontal area, and tissue is removed from another region called the insula.
- At the end of the operation, a silastic drain is left within the ventricle and the bone is replaced and secured with titanium plates and screws.
- The scalp is closed with absorbable stitches and a head wrap is applied.
After a hemispherotomy
After the operation, the child will be monitored in the Pediatric Intensive Care Unit (PICU) for one to two days, and an MRI will be performed to verify that all areas were disconnected appropriately. Over the course of the next few days, the patient will move to a normal neurosurgery room and undergo physical and occupational therapy.
The ventricular drain may be removed five to seven days after surgery, and a permanent shunting device is rarely required. Anticonvulsant medications are continued as seen fit by the treating neurologist, although it is often several months until medications are tapered.
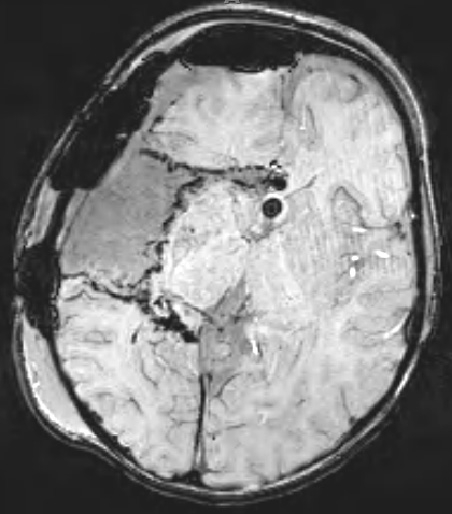
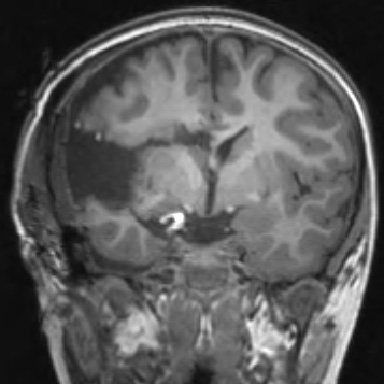
These MRI images show what a right-sided peri-insular hemispherotomy looks like.