What is midface hypoplasia?
Midface hypoplasia describes a situation in which the upper jaw, cheekbones and eye sockets have not grown as much as the rest of the face. Because of this, the eyes can seem large, appearing bulgy or “bug-eyed.” Also, the upper teeth usually do not meet the lower teeth well and result in an “under bite” appearance. This makes the lower jaw appear as if it is sticking out or more protrusive than usual. Finally, this can sometimes be so severe that people can develop severe snoring and sleep apnea, a situation in which someone cannot sleep well because they are waking up many times in the middle of the night due to lack of air.
So, I might have midface hypoplasia. Do I have to see a doctor?
Not necessarily. Many people can function normally with mild midface hypoplasia. Usually, these people have mildly prominent eyes and have teeth that do not meet well. Often, there is no problem with snoring or sleep apnea.
When should I consider treatment?
Treatment for midface hypoplasia may benefit those children and adults who have one or more of the following problems:
- Severe drying of the eyes (Keratoconjunctivitis): This can happen because the eyes are so protuberant (“bug-eyed”) that they are unable to close properly. Often, patients with this problem have been managing by placing ointment into their eyes at night in order to keep the eyes moist.
- The jaws do not meet correctly (Malocclusion): Many people may be able to get by with orthodontics which try to bring the upper teeth forward. However, in some circumstances, the gap between the upper and lower teeth is so large that surgery is needed to correct the problem.
- Obstructive sleep apnea (OSA): Individuals with bad sleep apnea can wake up hundreds of times a night and not even realize it. One associated sign is severe snoring. This is an indication that the tongue and tissues are hanging too far into the back of the throat, blocking the airway. Because they don't get a good night’s sleep, people with OSA can be tired all the time, falling asleep at work or school. There are also other negative side effects to this, including high blood pressure.
Who should be worried about midface hypoplasia?
Midface hypoplasia can affect anyone, including those with no medical problems whatsoever. It often has a familial predisposition – if your father had sunken cheekbones and bulgy eyes, you are likely to have it, too. However, people with the following diagnoses have a higher likelihood to have this problem:
- Craniofacial syndromes: Crouzon, Apert, Marshall-Stickler, Pfeiffer and similar disorders – These are all syndromes in which it is well-known that the skull and face do not grow normally.
- Cleft Palate – Some people with cleft palate do not have normal growth of the upper jaw.
- Achondroplasia (Achondroplastic dwarf) – Patients with this diagnosis not only have poor growth in their arms and legs, but the midface is also too small.
What can be done if I have this problem?
The good news is that this can be corrected with surgery. There are many different options available for treatment. First, you should be evaluated by a team of doctors who specialize in the treatment of midfacial hypoplasia. This team typically includes plastic surgeons (who specializes in craniofacial surgery), surgeons, dentists, orthodontists, learning and developmental specialists, and speech therapists. One such team exists at the Cleft Palate and Craniofacial Institute at St. Louis Children’s Hospital.
What kinds of operations are available?
Treatment will depend on the severity of the midface hypoplasia and the structures involved. For example, children with cleft palate and dental problems can often be treated with a procedure called a Le Fort I advancement – in which the upper jaw is moved forward to meet the lower teeth. Sometimes a double jaw (Le Fort I advancement + bilateral sagittal split osteotomy) must be performed. In this procedure, the upper jaw is moved forward and the lower jaw moved back so that the teeth can meet well. For children who have poor growth of the cheekbones and eye sockets in addition to a small upper jaw, a surgery called a LeFort III advancement can be performed. In this surgery, all of the bones of the upper face are brought forward, improving the position of the nose, eyes, upper jaw and teeth. Often, this will help to improve sleep apnea as well as facial appearance.
Some of the most severe cases of midface retrusion are treated by a procedure called distraction osteogenesis. This special technique allows the bones of the midface to be moved, over a period of time, into a better position. A metal piece, called a halo, is temporarily fixed to the skull bones, and the midface is pulled forward slowly following surgery to release the bones. Over the course of weeks, the face can be brought forward by even an inch or more. Later, with a minor procedure, the distractor can be removed.
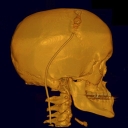
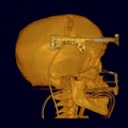

The above pictures depict pre-surgery (left), middle with distractor (center), and post-surgery (right).
You mention distraction osteogenesis. Is this only available for the upper jaw?
No. Distraction osteogenesis is a special technique that was originally developed to lengthen the bones of the leg. We are now able to use this technique to grow new bone and advance the length of the mandible (lower jaw), maxilla (upper jaw), midface (upper face including orbits) or skull.
I’m not a child. Who Should I call?
Many of our doctors treat adults as well, so please call 314.454.KIDS (5437) to request an appointment.









